Guidelines for Management of Monkeypox Disease
Guidelines for Management of Monkeypox Disease
Introduction
Monkeypox (MPX) is a viral zoonotic disease with symptoms similar to smallpox, although with less clinical severity. MPX was first discovered in 1958 in colonies of monkeys kept for research, hence the name ‘monkeypox.’ The first human case of monkeypox was reported from Democratic Republic of the Congo (DRC) in 1970.
Monkeypox Virus primarily occurs in Central and West Africa. In 2003, the first monkeypox outbreak outside of Africa was reported in the United States of America which was linked to contact with infected pet prairie dogs. These pets had been housed with Gambian pouched rats and dormice that had been imported into the country from Ghana.
Global Scenario
According to World Health Organization (WHO), in the present series of outbreaks being reported, this is the first time that chains of transmission are reported in Europe without known epidemiological links to West or Central Africa. Monkeypox has been reported as endemic in several other central and western African countries such as: Cameroon, Central African Republic, Cote d’Ivoire, Democratic Republic of the Congo, Gabon, Liberia, Nigeria, Republic of the Congo, and Sierra Leone. This has been also reported in certain non-endemic countries e.g. USA, UK Belgium, France, Germany, Italy, Netherlands, Portugal, Spain, Sweden, Australia, Canada, Austria, Canary Islands, Israel and Switzerland.
There are 4 reported cases of monkeypox virus in India as on 24 July 2022.
The World Health Organisation on 23 July 2022, recognizing the complexities and uncertainties associated with this public health event, has determined that the multi-country outbreak of monkeypox constitutes a Public Health Emergency of International Concern. During 14th August 2024, World Health Organisation (WHO) determined that the upsurge of mpox in the Democratic Republic of the Congo (DRC) and a growing number of countries in Africa constitutes a public health emergency of international concern (PHEIC) under the International Health Regulations (2005) (IHR).
Epidemiology
 Agent
Agent
Monkeypox virus (MPXV) is an enveloped double-stranded DNA virus that belongs to the Orthopoxvirus genus of the Poxviridae family. There are two distinct genetic clades of the monkeypox virus – the Central African (Congo Basin) clade and the West African clade. The Congo Basin clade has historically caused more severe disease and was thought to be more transmissible. The geographical division between the two clades has so far been in Cameroon - the only country where both virus clades have been found.
Host: Natural reservoir is yet unknown. However, certain rodents (including rope squirrels, tree squirrels, Gambian pouched rats, dormice) and non-human primates are known to be naturally susceptible to monkeypox virus.
Incubation period: The incubation period (interval from infection to onset of symptoms) of monkeypox is usually from 6 to 13 days but can range from 5 to 21 days.
Period of communicability: 1-2 days before the rash to until all the scabs fall off/gets subsided.
Mode of transmission:
- Human-to-human transmission is known to occur primarily through large respiratory droplets generally requiring a prolonged close contact. It can also be transmitted through direct contact with body fluids or lesion material, and indirect contact with lesion material, such as through contaminated clothing or linens of an infected person.
- Animal-to-human transmission: may occur by bite or scratch of infected animals like small mammals including rodents (rats, squirrels) and non-human primates (monkeys, apes) or through bush meat preparation.
Case Definition
Suspected case: A person of any age having history of travel to affected countries within last 21 days presenting with an unexplained acute rash AND one or more of the following signs or symptoms
- Swollen lymph nodes
- Fever
- Headache
- Body aches
- profound weakness
Probable case: A person meeting the case definition for a suspected case, clinically compatible illness and has an epidemiological link (face-to-face exposure, including health care workers without appropriate PPE; direct physical contact with skin or skin lesions, including sexual contact; or contact with contaminated materials such as clothing, bedding or utensils is suggestive of a strong epidemiological link).
Confirmed case: A case which is laboratory confirmed for monkeypox virus (by detection of unique sequences of viral DNA either by polymerase chain reaction (PCR) and/or sequencing).
Surveillance Strategies
The aims of the proposed surveillance strategy are to rapidly identify cases and clusters of infections and the sources of infections as soon as possible in order to:
- isolate cases to prevent further transmission
- provide optimal clinical care
- identify and manage contacts
- protect frontline health workers
- effective control and preventive measures based on the identified routes of transmission.
Surveillance outline
- Use Standard Case Definitions by all District Surveillance Units (DSUs) under Integrated Disease Surveillance Programme (IDSP) and at Points of Entry (PoEs).
- Even one case of monkeypox is to be considered as an outbreak. A detailed investigation by the Rapid Response Teams need to be initiated through IDSP.
- Report any suspected case immediately to the DSU/State Surveillance Units (SSUs) and CSU (Central Surveillance Unit), which shall report the same to Dte. GHS MoHFW.
- Send the samples as per the guidelines to the designated laboratories.
The salient features include:
- Targeted surveillance for probable case or clusters.
- Initiate contact tracing and testing of the symptomatic after the detection of the probable/confirmed case.
Core Surveillance Strategy
- Hospital based Surveillance: - Health facility-based surveillance & testing – in Dermatology clinics, STD clinics, medicine, paediatrics OPDs etc.
- Targeted Surveillance: This can be achieved by:
- Measles surveillance by Immunization division
- Targeted intervention sites identified by NACO for MSM, FSW population
Reporting
Reporting of cases to be done in the format as placed in Annexure 1.
Clinical Features
Monkeypox is usually a self-limited disease with the symptoms lasting from 2 to 4 weeks. Severe cases occur more commonly among children and are related to the extent of virus exposure, patient health status and nature of complications. The extent to which asymptomatic infection occurs is unknown. The case fatality ratio of monkeypox has historically ranged from 0 to 11% in the general population and has been higher among young children. In recent times, the case fatality ratio has been around 3-6%.
Common symptoms and signs
Prodrome (0-5 days)
- Fever
- Lymphadenopathy
- Typically occurs with fever onset
- Periauricular, axillary, cervical or inguinal
- Unilateral or bilateral
- Headache, muscle aches, exhaustion
- Chills and/or sweats
- Sore throat and cough
Skin involvement (rash)
- Usually begins within 1-3 days of fever onset, lasting for around 2-4 weeks
- Deep-seated, well-circumscribed and often develop umbilication
- Lesions are often described as painful until the healing phase when they become itchy (in the crust stage)
- Stages of rash (slow evolution)
- Enanthem- first lesions on tongue and mouth
- Macules starting from face spreading to arms, legs, palms, and soles (centrifugal distribution), within 24 hours
- The rash goes through a macular, papular, vesicular and pustular phase. Classic lesion is vesicopustular
- Involvement by area: face (98%), palms and soles (95%), oral mucous membranes (70%), genitalia (28%), conjunctiva (20%).Generally skin rashes are more apparent on the limbs and face than on the trunk. Notably the genitalia can be involved and can be a diagnostic dilemma in STD population
- By 3rd day lesions progress to papules
- By 4th to 5th day lesions become vesicles (raised and fluid filled).
- By 6th to 7th day lesions become pustular, sharpy raised, filled with opaque fluid, firm and deep seated.
- May umbilicate or become confluent
- By the end of 2nd week, they dry up and crust
- Scabs remain for a week before falling off
- The lesion heals with hyperpigmented atrophic scars, hypopigmented atrophic scars, patchy alopecia, hypertrophic skin scarring and contracture/deformity of facial muscles following healing of ulcerated facial lesions
- A notable predilection for palm and soles is characteristic of monkey pox
- The skin manifestation depends on vaccination status, age, nutritional status, associated HIV status. Monkeypox chiefly occurs in communities where there is often a high background prevalence of malnutrition, parasitic infections, and other significant heath-compromising conditions, any of which could impact the prognosis of a patient with MPX.
- The total lesion burden at the apex of rash can be quite high (>500 lesions) or relatively slight (<25).
Differential Diagnosis
Varicella (Chicken pox), disseminated herpes zoster, disseminated herpes simplex, measles, chancroid, secondary syphilis, hand foot mouth disease, infectious mononucleosis, molluscum contagiosum.
Complications
- Secondary infections
- Pneumonia, sepsis, encephalitis
- Corneal involvement (may lead to loss of vision)
Diagnosis
Personal Protective Equipment for handling the clinical specimens: PPE to be donned before collecting the specimens should include- Coveralls/Gowns, N-95 mask, Face shield/safety goggles, double pair of gloves. Donning & doffing of PPE should be carefully performed as per the standard procedure. Procedure for sample collection and transport of the clinical specimen are placed as Annexure 2. Instructions on sample packaging and transport are provided in detailed in Annexure 3.
Clinical samples to be collected from the cases as per the criteria mentioned below at Table 1:
| Traveller from outbreak /endemic region or Community Transmission | ||
| Asymptomatic |
|
|
| Symptomatic | Rash phase** | Recovery phase |
|
Urine in sterile urine container (3-5ml) |
|
Diagnostic modalities for Monkeypox with ICMR NIV Pune
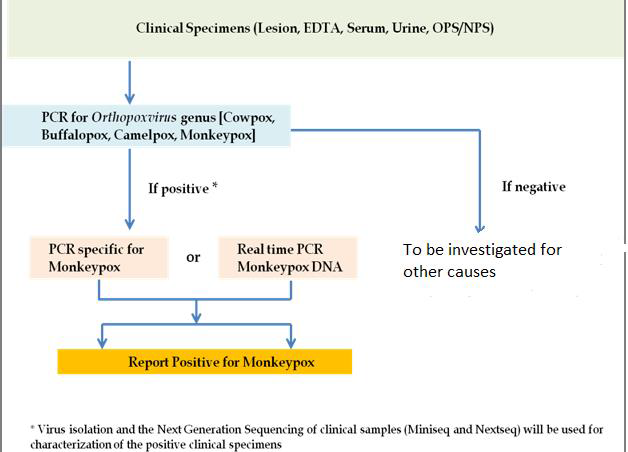
For the confirmation of Monkeypox on the suspected clinical specimens:
- PCR for Orthopoxvirus genus [Cowpox, Buffalopox, Camelpox, Monkeypox] will be done
- If specimen will show positivity for the Orthopoxvirus, it would be further confirmed by Monkeypox specific conventional PCR or real time PCR for Monkeypox DNA
- Additionally, virus isolation and the Next Generation Sequencing of clinical samples (Miniseq and Nextseq) will be used for characterization of the positive clinical specimens All the clinical specimens should be transported to the Apex laboratory of ICMR-NIV Pune routed through the Integrated Disease Surveillance Programme network of the respective district/state
All the clinical specimens should be transported to the Apex laboratory of ICMR-NIV Pune routed through the Integrated Disease Surveillance Programme network of the respective district/state
Contacts from ICMR-National Institute of Virology Pune Maharashtra, India for further queries related to collection and transportation of the clinical specimens
Maximum Containment Facility,
ICMR-NIV, Microbial Containment Complex,
130/1, Sus Road, Pashan, Pune 411021
Tel: Office: 020-26006111;
Management
Principles of Management
- Patient isolation
- Protection of compromised skin and mucous membranes
- Rehydration therapy and Nutritional support
- Symptom alleviation
- Monitoring and treatment of complications
Patient Isolation
- Isolation of the patient in an isolation room of the hospital/ at home in a separate room with separate ventilation
- Patient to wear a triple layer mask
- Skin lesions should be covered to the best extent possible (e.g. long sleeves, long pants) to minimize risk of contact with others
- Isolation to be continued until all lesions have resolved and scabs have completely fallen off
Supportive management of Monkeypox
| Component of management | Symptoms/Signs | Management |
| Protection of compromised skin and mucous membranes | Skin rash |
|
| Genital ulcers |
|
|
| Oral ulcers |
|
|
| Conjunctivitis |
|
|
| Rehydration therapy and nutritional support | Dehydration can occur in association with poor appetite, nausea, vomiting and diarrhoea |
|
| Symptom alleviation | Fever |
|
| Itching/Pruritus |
|
|
| Nausea and vomiting |
|
|
| Headache/ malaise |
|
Monitoring and treatment of complications
The patient should closely monitor for the appearance of any of the following symptoms during the period of isolation:
- Pain in eye or blurring of vision
- Shortness of breath, chest pain, difficulty in breathing
- Altered consciousness, seizure
- Decrease in urine output
- Poor oral intake
- Lethargy
In case any of the above symptoms appear, the patient should immediately contact nearby healthcare facility/ specialist.
Contact tracing
Definition of a contact
A contact is defined as a person who, in the period beginning with the onset of the source case’s first symptoms, and ending when all scabs have fallen off, has had one or more of the following exposures with a probable or confirmed case of monkey pox:
- face-to-face exposure (including health care workers without appropriate PPE)
- direct physical contact, including sexual contact
- contact with contaminated materials such as clothing or bedding
Contact identification
Cases can be prompted to identify contacts across household, workplace, school/nursery, sexual contacts, healthcare, houses of worship, transportation, sports, social gatherings, and any other recalled interactions.
Contact monitoring
- Contacts should be monitored at least daily for the onset of signs/symptoms for a period of 21 days (as per case definition above) from the last contact with a patient or their contaminated materials during the infectious period. In case of occurrence of fever clinical/lab evaluation is warranted.
- Asymptomatic contacts should not donate blood, cells, tissue, organs or semen while they are under surveillance.
- Pre-school children may be excluded from day care, nursery, or other group settings.
Health workers who have unprotected exposures to patients with monkeypox or possibly contaminated materials do not need to be excluded from work duty if asymptomatic, but should undergo active surveillance for symptoms for 21 days.
Advisory for International Passengers and surveillance at Airports and Role of APHOs/PHOs is also elaborated in Annexure 4.
Risk Communication and Preventive Measures
Raising awareness of risk factors and educating people about the measures they can take to reduce exposure to the virus is the main prevention strategy for monkeypox. There are number of measures that can be taken to prevent infection with monkeypox virus:
- Avoid contact with any materials, such as bedding, that has been in contact with a sick person.
- Isolate infected patients from others.
- Practice good hand hygiene after contact with infected animals or humans. For example, washing your hands with soap and water or using an alcohol-based hand sanitizer.
- Use appropriate personal protective equipment (PPE) when caring for patients.
Reducing the risk of human-to-human transmission
Surveillance and rapid identification of new cases is critical for outbreak containment. During human monkeypox outbreaks, close contact with infected persons is the most significant risk factor for monkeypox virus infection. Health workers and household members are at a greater risk of infection. Health workers caring for patients with suspected or confirmed monkeypox virus infection, or handling specimens from them, should implement standard infection control precautions. Samples taken from people and animals with suspected monkeypox virus infection should be handled by trained staff working in suitably equipped laboratories. Patient specimens must be safely prepared for transport with triple packaging in accordance with WHO guidance for transport of infectious substances.
Infection Prevention and Control (IPC)
A combination of standard, contact, and droplet precautions should be applied in all healthcare settings when a patient presents with fever and vesicular/pustular rash. In addition, because of the theoretical risk of airborne transmission of monkeypox virus, airborne precautions should be applied as per risk assessment.
Clinical triage includes early recognition and immediate placement of patient in separate area from other patients (source control). All individuals, including family members, visitors and HCWs should apply standard, contact and droplet precautions.
Patient isolation
Patient should be managed in isolation, precautions should be taken to minimize exposure to surrounding persons, which include placing a surgical mask over the patient’s nose and mouth—if tolerable to the patient—and covering any of the patient’s exposed skin lesions with a sheet or gown.
Ambulance Transfer
- When a case has to be transported, the personnel accompanying the patient should wear PPE (long sleeved gown, N95 mask, gloves, and goggles).
- Give prior information to the hospital of the admission/transfer of a potentially infectious person.
- Request patient to wear a mask (if tolerated) and advise on Respiratory Hygiene and Cough Etiquette.
- If lesions are present, cover them with long sleeved clothing/pant or a clean sheet to minimize contact with others. In the ambulance use disposable linen if available.
- The ambulance should be cleaned and disinfected before using for the other patients. After wearing PPE, surfaces (stretcher, chair, door handles etc.) should be cleaned with a freshly prepared 1% hypochlorite solution or equivalent. Carefully place reusable blankets in a bag without shaking or fluffing them, then put into a laundry bag and send for laundering clearly labelling it so that person in the laundry wears appropriate PPE before handling or autoclaves it before opening. Follow manufacturer’s instructions for cleaning/disinfecting reusable equipment in the ambulance. All masks and any waste contaminated with crusts, secretions, serum or body fluids should be disposed of as infectious waste in yellow bag. In the ambulance, if the driver’s chamber is not separate, driver should also use PPE.
Additional Precautions
- PPE (Disposable gown, gloves, N95 mask, Eye goggles) should be donned before entering the patient’s room and used for all patient contact. All PPE should be disposed of prior to leaving the isolation room where the patient is admitted.
- Hand hygiene (following standard steps of hand hygiene) after all contact with an infected patient and/or their environment during care.
- Correct containment and disposal of contaminated waste (e.g., dressings) in accordance with Biomedical Waste Management guidelines (2016 & subsequent amendments) for infectious waste.
- Care when handling soiled laundry (e.g., bedding, towels, personal clothing) to avoid contact with lesion material.
- Soiled laundry should never be shaken or handled in manner that may disperse infectious particles.
- Care when handling used patient-care equipment in a manner that prevents contamination of skin and clothing.
- Ensure that used equipment has been cleaned and reprocessed appropriately.
- Ensure provisions are in place for cleaning and disinfecting environmental surfaces in the patient care environment.
- Hospital disinfectant currently used for environmental sanitation may be used as per recommendations for concentration, contact time, and care in handling.
IPC at home
Patients who do not require hospitalization may be managed at home taking following preventive measures:
- Patients should be isolated in a room or area separate from other family members. Healthy household members should limit contact with the patient.
- Patients should not leave the home except for medical care.
- No visitors should be allowed at home.
- Patients, especially those who have respiratory symptoms (e.g., cough, shortness of breath, sore throat) should wear a surgical mask. If this is not feasible, other household members should consider wearing a surgical mask when in the presence of the patient.
- Disposable gloves should be worn for direct contact with lesions and disposed of after use.
- Skin lesions should be covered to the best extent possible (e.g., long sleeves, long pants) to minimize risk of contact with others.
- Contain and dispose of contaminated waste (such as dressings and bandages) in the Biomedical waste disposable bag Do not dispose of waste in landfills or dumps.
- Proper hand washing with soap and water (or use of an alcohol-based hand rub) should be performed by the patient and other household members after touching lesion material, clothing, linens, or environmental surfaces that may have had contact with lesion material.
- Laundry (e.g., bedding, towels, clothing) may be washed with warm water and detergent;
- Care should be used when handling soiled laundry to avoid direct contact with contaminated material.
- Soiled laundry should not be shaken or otherwise handled in a manner that may disperse infectious particles.
- Dishes and other eating utensils should not be shared. Soiled dishes and eating utensils should be washed with warm water and dish washing soap.
- Contaminated surfaces should be cleaned and disinfected. Standard household cleaning/disinfectants may be used in accordance with the manufacturer’s instructions.
- Pets and domestic animals should be excluded from the patient’s environment.
Duration of Isolation Procedures
Affected individuals should avoid close contact with immunocompromised persons and pregnant women until all crusts are gone. Isolation precautions should be continued until all lesions have resolved and a fresh layer of skin has formed.
Risk Communication
This includes providing public health advice through the channels that target audiences use on how the disease transmits, its symptoms, preventive measures and what to do in case of suspect or confirmed infection. This should be combined with targeting community engagement to the population groups who are most at risk, working closely with health care providers, including STD clinics, and civil society organizations.
Risk communication should be informed by insights from social listening detecting public sentiment and should timely address possible rumours and misinformation. Health information and advice should be provided avoiding any form of stigmatization of certain groups such as men who have sex with men (MSM).
The key measures that can be taken to prevent infection with monkeypox virus:
- Isolate infected patients from others who could be at risk for infection.
- Avoid contact with any materials, such as bedding, that has been in contact with a patient of Monkeypox.
- Practice good hand hygiene after contact with infected persons. For example, washing your hands with soap and water or using an alcohol-based hand sanitizer.
- Use masks and gloves when caring for patients.
Last Modified : 8/19/2024
Provides information about Monkeypox.
Provides information on the concept - One Health a...
This topic provides information about Echinococcos...
Provides information about Marburg Virus Disease