Stress During Disasters
Stress During Disasters
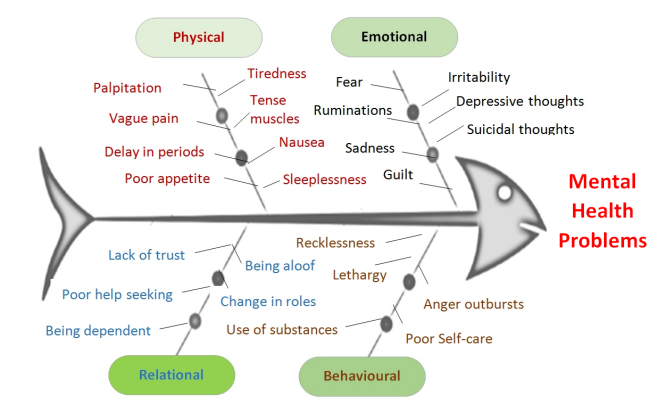
- Physical Reactions
- Behavioural Reactions
- Psychological/Emotional Reactions
- Relational Reactions
- Multiple reactions experienced by different age groups in the post-disaster phase
- Reactions among Children
- Reactions among Adolescents
- Reactions among adults
- Reactions among older adult
- Dealing with the Psychological Reactions among Different Age Groups
 One of the salient features of psychosocial care is enabling disaster survivors to understand stress and its reactions. The unpredictable environment, unexpected living conditions and unpleasant experiences cause excessive distress.
One of the salient features of psychosocial care is enabling disaster survivors to understand stress and its reactions. The unpredictable environment, unexpected living conditions and unpleasant experiences cause excessive distress.
Traumatic experiences yield anxiety and stress when it exceeds the coping capacity and resources of the individual, family and community. If people understand the reactions caused by the disaster, it is easy for them to deal with the changes caused by it.
Numerous reactions are generated by stress and its manifestations. This varies from person to person during different phases of disaster. Prior knowledge about the stressful reactions and its consequences helps both the disaster survivor and the caregiver to identify the body's response to stress. This also facilitates early identification and quick treatment during the response, relief and rehabilitation phases.
Physical Reactions
Physical reactions are easily noticeable. One of the most common physical symptoms, experienced by disaster survivors is body pain/aches. For relief from pain, people visit doctors or take self-prescribed medicines. Mostly, psychological reactions experienced by disaster survivors are portrayed as physiological reactions such as tension, fatigue, restlessness, disturbances in sleep and appetite, body pain/ache, muscle cramps, variations in blood sugar/pressure levels and rapid startle reactions. Some examples of physical reactions are given below:
- Stomach ache and change in appetite
- Headache
Behavioural Reactions
Stress caused due to traumatic experiences, when goes beyond the coping capacity of a person lead to adaptive and maladaptive behaviours. Some of the common maladaptive behaviours are: lack of interest in life, reduced energy/activity level, excessive consumption of substances (alcohol, tobacco etc), isolating self from persons, places or environment.
- Change in behaviour
- School refusal
Psychological/Emotional Reactions
Psychological or emotional reactions are subjective experiences. There may be change in the person’s behaviour, emotional expressions, and thinking patterns. For instance; trouble in concentrating, confusion, issues with memory, difficulty in making decisions and problem solving, anger, irritability, fear, anxiety, repetitive thoughts, suicidal thoughts/attempts, forgetfulness, grief, guilt, lack of interest, hopelessness, worthlessness and helplessness etc. Like physical or behavioural reactions, psychological reactions might not be visible. All the other reactions would eventually lead to a psychological reaction and vice versa.
- Despair about losses
- Helplessness, sadness and guilt
- Nightmares
Relational Reactions
Stress can have significant impact on the relationships. It makes the person avoid or increase interactions with others. This would affect the person’s social support and help-seeking behaviour. Change in roles and responsibilities post disaster would impact the family or community interaction patterns. Interpersonal reactions include trust issues, increased conflicts, feeling of rejection or abandonment, not accepting/judging others and exercising control over others.
- Change in interaction
- Being aloof
Multiple reactions experienced by different age groups in the post-disaster phase
(Adapted from NSWHealth, 2000)
Reactions among Children
- Physical: Poor bowel or bladder control, difficulties in speech (stuttering, baby talk), poor or increased appetite, physical complaints (headache, stomach pain).
- Behavioural: Inactiveness, thumb sucking, throwing temper tantrum, aggression, school refusal/avoidance.
- Psychological: Fear (new circumstances, being separated, dark, animals, weather, safety), irritability, nightmares, poor attention, poor concentration, lack of interest, preoccupation and thinking about the events related to the disaster.
- Relational: Not leaving parents, seeking parental attention, not mingling with peers.
Reactions among Adolescents
- Physical: Problems with sleep and food intake, pain/ache in the body.
- Behavioural: Rebelliousness, issues at school (quarrelling, picking up fights, poor interest in studies), increased or decreased activity/energy, engaging in unlawful/criminal behaviour, using drugs/alcohol.
- Psychological: Non-responsiveness, mood swings.
- Relational: Seeking attention, poor prosocial behaviour, displaying avoidant behaviour, change in peer groups.
Reactions among adults
- Physical: Sleep disturbances, poor/increased appetite, feeling tired or exhausted, somatic problems (gastrointestinal, multiple body pain, worsening of existing medical/psychiatric conditions).
- Behavioural: Avoiding (person/place), increased/decreased activity, anger outbursts, using substances.
- Psychological: Sadness, continuous crying, feeling sad, anxious, guilty, being irritable, fearful, having depressive thoughts (hopelessness, worthlessness, helplessness), having mood swings, self-blame/doubt.
- Relational: Frequent family conflicts, self- isolation from others.
Reactions among older adult
- Physical : Worsening of chronic medical/psychiatric conditions, change in sleep and eating patterns, decline in physical health.
- Behavioural : Agitation/irritability.
- Psychological : Feeling depressed, disoriented, having confusion, memory problems, poor interest, being suspicious, feeling of despair, being anxious about unfamiliar environment, feeling of embarrassment.
- Relational : Withdrawn behaviour, adjustment issues.

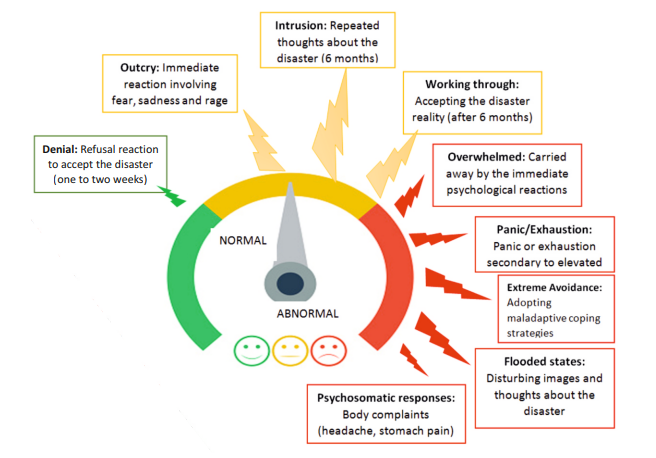
All of these reactions are normal reactions to a disaster. Survivors experience different emotional reactions during different phases of disaster. Understanding the variations in the psychological reactions over different time intervals and differentiating between normal and abnormal reactions help in developing appropriate psychosocial or mental health interventions. The figure below helps in understanding the distinction between normal and abnormal reactions during the disaster cycle.
Dealing with the Psychological Reactions among Different Age Groups
Children (1 to 5 years)
- Provide simple and direct messages.
- Provide verbal reassurance and appropriate physical touch.
- Help in restarting and following the daily routine.
- Make the child to name the emotions she/he is experiencing.
- Facilitate living with family or with familiar and safe individuals/environment.
- Reduce or eliminate images/news/sounds/persons that remind the disaster.
- Encourage the child to talk about the feelings (especially the losses).
- Create opportunities for active play or group activities.
- Make sure that the child knows that you can be approached for help in times of distress.
Children (6 to 11 years)
- Reduce home/school expectations from the child.
- Enable structured but flexible activities at home/relief camp.
- Encourage the child to talk about his/her traumatic feelings.
- Actively listen to the child with warmth and care.
- Provide authentic information and correct misconceptions. l Create peer activities using expressive arts.
- Have an eye on the needs of special children.
- Educate on safe/unsafe touch.
- Make the child know that there is help always.
- Monitor the child’s screen time.
Adolescents
- Set the realistic home/school expectations.
- Facilitate sharing traumatic experiences.
- Ensure confidentiality.
- Do not force to talk.
- Create routine involving physical activities, self-care activities, group meeting and other social activities.
- Do not confront behaviour/feelings.
- Connect the adolescents’ impulsivity or reckless behaviour to the disaster event.
- Educate on staying away from psychoactive substances. (alcohol, tobacco or other drugs), risky sexual behaviour, abuse and other social evils.
- Regulate the adolescent’s screen time.
- Provide information of healthy coping, whom to approach in times of distress/crisis.
- Take care of adolescents with special needs (persons with disability, history of child sexual abuse, abandoned, orphaned, etc.).
Adults
- Enable access to essential resources.
- Create channels for the adult to talk about the disaster experiences.
- Provide authentic information on services, systems and aid.
- Correct false information.
- Help them to improve their problem-solving abilities.
- Encourage direct and frequent communication between family members.
- Provide information on strategies to follow while being with their spouses, children or older adults in the family.
- Empower the adults on the adaptive coping strategies and discourage maladaptive patterns.
- The community is the first responder in any disaster so empower the adult to take care of themselves and the community.
- Assess for abnormal reactions and facilitate appropriate mental health services.
Elderly
- Provide verbal and physical reassurance.
- Ensure access to essentials.
- Help in sustaining or rebuilding the support systems.
- Enable easy access to medical and financial resources.
- Create avenues to express their traumatic experiences.
- Educate on elderly abuse.
- Provide legal options available in case of elderly abuse.
Last Modified : 11/23/2023
Tips for handling mental issues during pandemics/d...
Ministry of Social Justice & Empowerment's 24x7 To...
MANODARPAN initiative of Ministry of Education is...
World Suicide Prevention Day (WSPD), on 10 Septemb...